:sharpen(level=0):output(format=jpeg)/up/dt/2024/07/Shutterstock_1051488260.jpg "Endodontic and surgical option to inner root resorption")
There are two sorts of IRR: inflammatory and alternative. The primary normally has a spherical and common form, and the second one sort could also be misdiagnosed as exterior cervical resorption owing to the equivalent form. An important a part of remedy is the removal of the essential apical pulp tissue maintaining the IRR. If the IRR has no longer perforated the foundation wall, most effective root canal remedy must be carried out; alternatively, the presence of root wall perforations in some circumstances may additionally require a surgical manner.
. Coronal plane showing the lesion (b). Sagittal plane showing the perforation of the cortical bone (c).")
Case 1—Figs. 1a–c: CBCT scan taken sooner than the remedy. Axial airplane appearing the foundation wall perforation (a). Coronal airplane appearing the lesion (b). Sagittal airplane appearing the perforation of the cortical bone (c).
Case 1
A 40-year-old feminine affected person used to be referred to the endodontic place of work as a result of an incidental discovering of IRR within the maxillary left lateral incisor on a breathtaking radiograph. A CBCT scan used to be taken to evaluate the level of the resorption, devise a remedy plan and resolve the diagnosis (Figs. 1a–c). The resorption hollow space used to be positioned in the midst of the foundation and had perforated the mesial wall of the foundation. The reasonably spherical and common form of the resorption indicated the inflammatory sort. The osteolytic focal point instructed a lesion used to be provide subsequent to the perforation house (Fig. 2). Owing to the dimensions of the wall perforation and the presence of the lesion, the remedy plan concerned a single-session root canal remedy in addition to a surgical manner.
After acting native anaesthesia, the get admission to hollow space used to be created. The pulp chamber used to be reshaped with an ultrasonic diamond-coated tip. The pulp chamber used to be wiped clean with sodium hypochlorite, and the pulp tissue used to be partly got rid of from the foundation canal. An incision used to be produced from the frenulum, in the course of the gingival sulcus from the maxillary first incisor to the maxillary dog. After elevating a flap, the granulation tissue used to be got rid of from the resorption hollow space with a small excavator.
The foundation canal shaping protocol used to be carried out with typical chemomechanical preparation. The shaping series used to be guided by way of preliminary negotiation the usage of passive hand recordsdata, adopted by way of preparation with rotary recordsdata and irrigation the usage of sodium hypochlorite, activated with guide needle agitation. After the foundation canal shaping process, the next irrigation protocol used to be carried out: 3 mins of alternating irrigation and ultrasonic agitation of five.25% sodium hypochlorite, smear layer removing with double alternating irrigation with EDTA 17% and sodium hypochlorite, and 5 mins of alternating irrigation and ultrasonic agitation of sodium hypochlorite. All the way through all of the instrumentation and irrigation procedures, the suction used to be positioned subsequent to the resorption hollow space to keep away from inflammation of the bone and surrounding tissue.
The obturation of selection used to be heat vertical compaction of gutta-percha and sealing with the bioceramic sealer CeraSeal (Meta-Biomed; Fig. 3). The resorption hollow space used to be stuffed with Biodentine (Septodont; Figs. 4a & b), and the coronal a part of the foundation canal used to be stuffed with heat gutta-percha. The flap used to be repositioned and sutured, and the enamel used to be restored with composite resin.
Recall appointments have been carried out after 5 and 6 months (Fig. 5). The bone therapeutic used to be entire after 5 months (Figs. 6a-c), and after 30 months, there have been no indicators of the bone defect, fracture or every other abnormalities (Figs. 7a & b).
Case 2
A 28-year-old affected person used to be referred to the endodontic place of work after prognosis of inflammatory IRR within the maxillary proper central incisor on a periapical radiograph. A CBCT scan used to be taken to resolve the diagnosis and to devise the remedy (Figs. 8a-e). The 3-d symbol published perforation of the labial wall of the foundation and destruction of the package deal bone surrounding the resorption hollow space.
An incision used to be produced from the maxillary left central incisor in the course of the gingival sulcus to the best maxillary dog. After elevating a flap, the granulation tissue used to be got rid of from the resorption hollow space with a small excavator (Figs. 9–11). The foundation canal shaping protocol used to be carried out with typical chemomechanical preparation. The shaping series started with negotiation with passive hand recordsdata, adopted by way of preparation with rotary recordsdata and irrigation the usage of sodium hypochlorite with guide needle agitation. The irrigation protocol used to be carried out as described in Case 1.
The obturation of selection used to be heat vertical compaction of gutta-percha and sealing with the AH Plus sealer (Dentsply Sirona). The resorption hollow space used to be stuffed with a fast-setting mineral trioxide mixture (Harvard Dental), the coronal a part of the foundation canal used to be stuffed with heat gutta-percha and collagen sponge used to be positioned (Figs. 12a & b; Figs. 13a & b). The flap used to be repositioned and sutured, and the enamel used to be restored with the GRADIA composite resin (GC; Figs. 14a & b, Fig. 15).
Recall appointments used to be carried out after two (Figs. 16a & b) and 4 years (Figs. 17a & b). The radiographic exam confirmed the presence of package deal bone. The periodontal standing used to be solid, and the enamel remained asymptomatic.
Dialogue
Even though the aetiology of IRR stays unclear, research agree that casting off the essential pulp from the apical house is a very powerful to halting the resorption. Research additionally concur that when the inner resorption has been stopped, there’s little chance that the method will revive. Thus, one of the essential prognostic components is the restorability of the enamel. Within the circumstances introduced, the biomechanic integrity of the enamel used to be compromised, however the sufferers’ age and resolution have been crucial components for remedy making plans.
The 2 sorts of IRR, inflammatory and alternative, have quite other mechanisms of development, however each contain the task of osteoclasts. Then again, from the scientific viewpoint, the glory between the 2 sorts isn’t important.
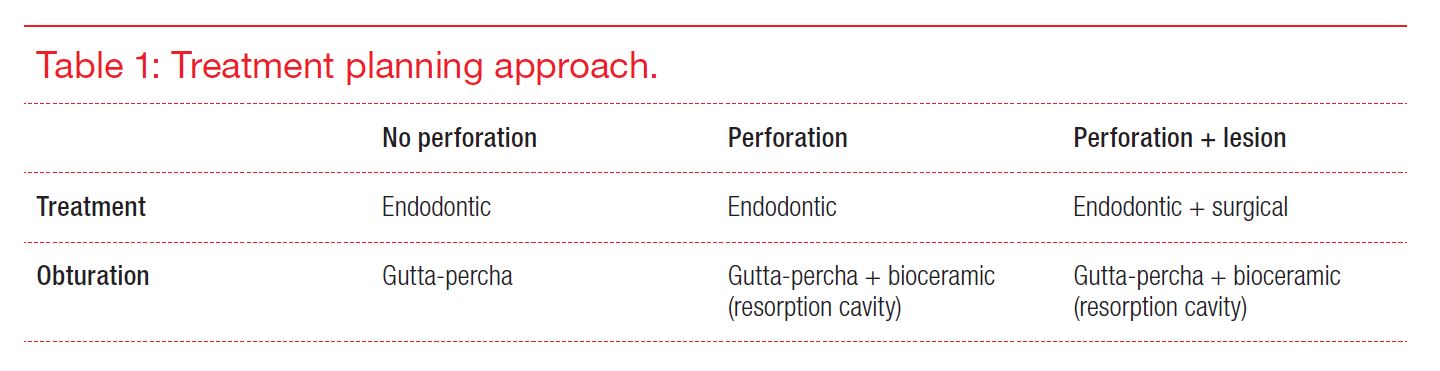
So as to diagnose IRR, it is suggested to take a CBCT scan. 3-d diagnostics is a very powerful for developing the remedy plan. The form of the realm of resorption and perforation of the foundation wall are crucial components for figuring out the remedy making plans manner (Desk 1). The circumstances introduced have demonstrated {that a} mixed endodontic and surgical manner is the best option for circumstances of IRR that has perforated the foundation wall and is related to a lesion or destruction of the encircling bone.